
Check out the calculator below!
Hypernatremia
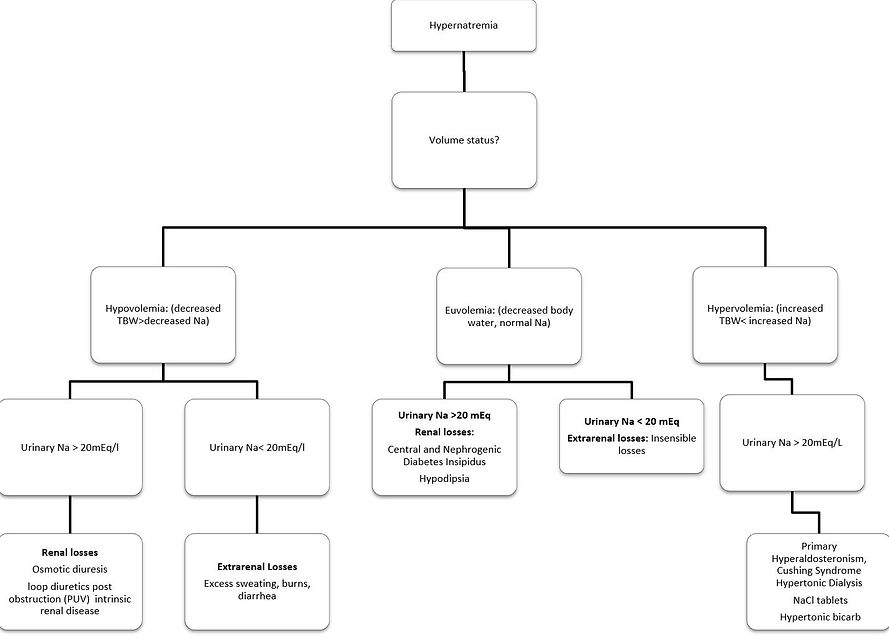
Conceptually similar to hyponatremia, hypernatremia is almost always a function of (too little) water. In hypernatremic dehydration, for example, there is a loss of water>loss of salt.
See the diagnostic algorithm and calculators below. One thing to point out is even though a patient is hypernatremic, if they are hypovolemic, the kidneys are trying to restore intravascular volume, so urine Na is low. As opposed to hyponatremia, hypernatremia is ALWAYS hyperosmotic.
Management:
-
We must replace daily needs (see section, "Fluids and Electrolytes"), as well as losses.
-
Daily needs:
-
Maintenance
-
-
Losses:
-
Total fluid deficit can be estimated or ideally, a recent weight change, where 1kg lost=1L (1000ml).
-
-
Total fluid deficit can then be subdivided into:
-
Free water is to be replaced so as not to exceed a decrease in serum sodium >0.5mEq/L per hour (12mEq/L per day) to avoid cerebral edema
-
One question we get is about DI. DI is either a defect in production of ADH (Central- craniopharyngioma, septo-optic dysplasia, infiltrative disease etc.) or response to ADH in the distal tubule (AVP or AQP2 receptor defect (genetic), decreased trafficking to the membrane, decreased function (medications such as lithium, amphotericin, cisplatin). Diagnosis needs to include elevated serum osmolality with decreased urine osmolality, (typically <300mOsm/kg) and elevated urine sodium (vs. SIADH which has elevated urine osmolality and elevated urine sodium). If it is a central defect, desmopressin has a role (looking for osmolality increase >50%). If it's peripheral (kidney), there are various options: decreasing solute load, thiazides (increase proximal absorption after an initial diuretic effect), NSAIDs, etc.
-
The hourly rate of fluid replacement + maintenance for a patient with sodium derangements based on calculations can be extremely high. We therefore often max out our fluid rates at around 1.5x Maintenance (calculated fluids vs suggested fluids). If your patient can tolerate PO as well, that may be another option to get additional fluid as well.
-
Free Water deficit (=0.6 * wt in Kg (current Na/140- 1)), and
-
Isotonic losses (since the patient lost some sodium and other electrolytes as well)
Differential diagnosis:
DI with urine osm <300mOsm/kg
Calculator
Time to return to 140 mEq/L
Daily Maintenance, ml
Total Fluid Deficit,ml
**Free Water Deficit, ml**
Isotonic loss, ml
Daily Maintenance, ml
Total Fluid Deficit, ml
Free water deficit, ml
Isotonic loss, ml
**Free water deficit return in the first 24 hrs:**
If time to return <=24 hrs - will return full free water deficit
If time to return >24 but <36hrs - will return 2/3
If time to return >=36 hrs - will return 1/2
(slow rate to avoid cerebral edema)
Remaining fluid balance after bolus
Remaining fluid balance after bolus
Description | H₂O | Na |
|---|---|---|
Inspiration and credit for the calculator: Dr. Alexandra Mazo
Suggested readings:
- https://www.uptodate.com/contents/hypernatremia-in-children
Calculator components:
- Maintenance: Holliday- Seager method, see "Fluids and Electrolytes"
- Fluid deficit: 1ml:1gm lost
- Free water deficit: 0.6 x Baseline wt (Current Na/140-1)*1000
- Isotonic loss: is equal to 154mEq/L