
Dialysis Basics
Many residents are mystified and scared by the concept of dialysis. While the topic is extensive and somewhat complicated, the basics of dialysis are actually fairly straightforward, but it is easy to get caught up in the verbiage. Here we discussed the mechanisms and types of dialysis, along with some practical knowledge when looking at an order set or treating a patient who is receiving dialysis.
1. What Dialysis Replaces
Dialysis the way it is used is in a way a misnomer. The term technically refers to clearance (the definition of dialysis is to loosen apart), but it is often used to include both clearance and fluid removal.
2. How Does Dialysis Work? (Tea vs Coffee)
As noted above, one can accomplish clearance in two ways, diffusion and convection
Diffusion
Occurs when solutes move from high concentration → low concentration. The comparison is to making tea- the tea diffuses out of the teabag into the water
Example:
-
Blood urea: 80
-
Dialysate urea: 0
Urea diffuses across the membrane to reach
equilibrium.
Convection
Water is pushed across the membrane
and drags solutes with it. The comparison
is to coffee- you compress the grounds and
force them through the grounds
along with water to make coffee.
Better for removing:
-
Cytokines
-
Larger molecules
Dialysis modalities
Broadly, there are two modalities of dialysis: hemodialysis and peritoneal dialysis. The goals of dialysis (fluid removal and clearance), while occurring in different ways, is the common theme across all modalities.
3. Hemodialysis (HD)
Hemodialysis uses an artificial dialyzer membrane.
Blood leaves the patient → enters the dialyzer → passes through tons (thousands!) of thin tubes that have a semipermeable membrane while dialysate flows on outside at a predefined concentration of sodium, potassium, urea, etc. to create that concentration gradient (i.e. dialysis). (see image above).
Ultrafiltration
-
Removes excess fluid by exerting a pressure on the blood from one side of the membrane to the other as well as some electrolytes, but less than diffusion. Therefore, one can only do an UF session with some electrolyte changes but not as significant as with dialysis. This is useful if someone only needs/needs more fluid removal.
Typical HD session:
-
3–4 hours
-
3-4 times per week typically.
Advantages (vs PD in chronic patients).
Fewer hours attached to a machine
Fewer times a week
No need for equipment at home
Disadvantages
Have to go to an HD center at a particular time 3-4 times a week for 3-4 hours at a time
Fluid shifts are significantly more and some patients don’t tolerate it all that well.
More of an option for older children who are not on a total liquid diet as there is only so much fluid to remove in one session
Below is a sample HD prescription. This is a prescription for someone who may come 3 or 4 times a week. the dialysate flow rate is typically a 2:1 ratio to the blood flow rate to maximize diffusion. We remove fluid to a target weight (EDW= estimated dry weight) to prevent complications of fluid overload. Access is via AV fistula.
Aside: some patients do make significant amounts of urine but the renal function requires them to be on dialysis. some patients need very little fluid removal. some patients who have slightly better function may only need HD twice a week.
HD prescription
K+: 2 mEq
Ca++: 3.5 mEq
Bicarb (mEq): 37
Na+: 140 mEq
Dialyzer: F180
Dialysate Temperature (C): 37
Blood Flow Rate -As tolerated to a maximum of: 350 mL/min
Dialysis Flow Rate: 700 mL/min
Duration of Treatment: 3 Hours
Dry weight (kg): 60kg
Goal Fluid to remove: to Estimated Dry Weight
Tubing: Adult combiSet
Laterality: Right
Access Site: AVF
4. Continuous Renal Replacement Therapy (CRRT)
CRRT is the overarching terminology given to extracorporeal kidney therapy that is run at slower rates than HD. , CRRT is used in ICU patients who may not tolerate HD for typically one of two reasons (or both). There are other reasons as well, but these are two of the most common.
-
Hemodynamic instability- The blood flow of CRRT that goes from patient to machine is typically run slower than HD circuits
-
Volume requirements: patients in the ICU receive feeds/TPN, antimicrobials/antifungals, pressors etc where the volume that the patient is getting is too large to remove with HD (which only runs 3-4 hours/session and there is only so much fluid you can remove in one session).
The CRRT circuit typically runs continuously over 24 hours
and allows gentle fluid removal. As mentioned earlier, we can
“clean” the blood with diffusion or convection.
With many machines you can do CVVH, CVVHD, or both (CVVHDF).
Much of choice of modality depends on machine capabilities
and center experience.
The machine setup can be a bit confusing,
but the important points are thus:
CVVH involves convection, i.e. exerting a pressure
to achieve fluid removal. If this is the only way one is
removing solutes and toxins, then the rates will have to
be fairly high, on say an average ~ 40ml/kg/hr of fluid
and solute removal. You can imagine, after just a few
hours a patient can become volume depleted and have
“wonky” electrolytes fairly rapidly. Therefore, we provide
what is called replacement fluids- typically a standard
out of the box fluid that contains electrolytes that is given
back to the patient to maintain their fluid volume
(you set the rate of fluid removal on the machine that
takes the replacement rate into account, e.g. if
replacement rate is 100ml/hr you program the machine
to remove 150ml/hr to achieve fluid removal). This fluid has two different location to be given back to the patient and is infused in different areas of the machine to achieve specific outcomes, but that is beyond the scope of this primer (see above image).
CVVHD involves diffusion only, i.e. standard out of the box dialysis fluid is run countercurrent flow to blood flow moving through a semipermeable membrane (similar to HD) at a specific rate with pressure placed on the blood flow in the filter to achieve fluid removal.
CVVHDF is the combination of both, which we do at my center. In which case, we divide our total desired clearance between the two modalities running concurrently (diffusion with dialysate fluid and convection achieved through transmembrane pressure in the filter with replacement fluid given back to the patient) to achieve CRRT.
Below is a simplified sample prescription of a patient receiving CRRT-CVVHDF
The filter size is dependent on body surface area.. The dialysate fluid comes in various concentration of Ca++ and K+ (in addition to other electrolytes), in this case we are using a bag with 4mEq/l of potassium and 2.5meq/L of Calcium (physiologically active calcium) for dialysis/dialysate (does not come in contact with the patient, see image) and Prismasol as replacement fluid (since we are using convective therapy, see image). Clearance rates are divided between dialysis and convection therapies.
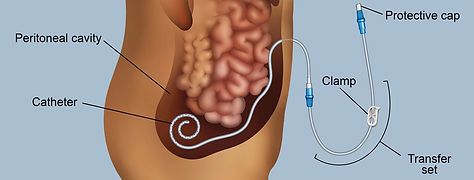
5. Peritoneal Dialysis (PD)
Although PD is a different modality, the concepts are similar.
We need to:
1) remove fluid and 2) provide clearance. This can be used in the acute or chronic setting.
Peritoneal dialysis uses the peritoneal membrane as the dialysis membrane. Dialysate fluid is placed inside the abdomen.
Solutes move between:
-
Blood in peritoneal capillaries
-
Dialysate in the peritoneal cavity
To achieve fluid removal and solute clearance, we need to have diffusion and convection.
Diffusion
-
Removes electrolytes and toxins. see sample prescription below. The dianeal bags contain sodium, magnesium, calcium, lactate (as a base)
Osmosis (i.e. UF)
-
Removes water via glucose osmotic gradient. If you recall the osmotic equation (2NA + BUN/2.8 + Glucose/18) glucose is osmotically active (remember DKA and HHS!). the dianeal contains 1.5% glucose (15g/L, Osmolality 346mOsm/L) even 4.25% glucose (42.5g/L= 485mOsm/L) which exerts an osmotic draw and removes fluid.
5a. PD Cycle
The cycle then repeats.
Dialysis can occur via:
-
Manual exchanges (CAPD)
-
Automated cycler (CCPD/APD)
Advantages of APD
Can be done at home, typically overnight for 7-12 hours
A bit more “gentle” than HD, but one can overdo it on the prescription
Good for those on liquid diets and who are anuric as the therapy is nightly vs HD
Disadvantages
One needs space to hold a lot of equipment – the cycler, bags, supplies etc
A trained caregiver needs to learn how to use the cycler, attach the patient, and understand warning signs as well as troubleshooting.
In our institution we typically do CCPD using a cycler (see image with fluid above). This mean a patient will have a machine at home. Each fill-dwell-drain is one cycle. Patients typically require multiple cycles over 7-12 hours. Manipulating the cycles and time is a bit beyond the scope of this primer, but a starting PD prescription for a child is around 5 cycles over 7 hours and adjustments are made from there.
Below is a sample PD prescription. There are other components that have been removed, but this is the basic idea.
Dialysate #1: 1.5% Low Ca
Total dialysate volume (ml): 5000
therapy time (hours): 7
therapy time (minutes): 420
fill volume (ml): 1,000
Baxter last fill volume (ml): none
# of cycles: 4
Baxter patient weight: 19.5
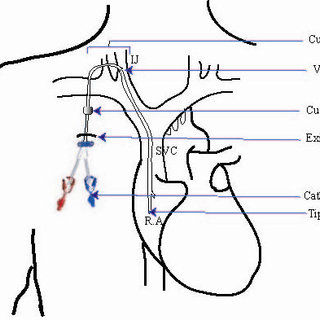
6. Hemodialysis Access
Temporary HD Catheters
Common sites:
-
Internal jugular
-
Femoral
Avoid:
-
Subclavian due to the possibility of developing central vein stenosis and then be unable to place permanent HD catheter
Permanent Access
AV Fistula
Best long-term option. It takes 4-6 weeks to be able to use it after placement, so sometime patients receive a catheter first as they wait for the fistula to mature.
Advantages:
-
lowest infection risk
-
longest survival
Tunneled HD Catheters
Used when fistula not available (patient too small etc). Ideally placed in Internal Jugular vein
HD catheters differ from regular central lines:
Feature Reason
Larger diameter High blood flow
Dual lumen Simultaneous inflow/outflow
Special (thicker) material Prevent collapse
7. PD Access
Tenckhoff Catheter
Features:
-
silicone
-
cuffs to prevent infection
-
tunneled exit site
This catheter made long-term PD possible in children.



Replacement fluid
Dialysate
Effluent (UF)



Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2).
Dialysis Catheters and Their Common Complications: An Update - Scientific Figure on ResearchGate. Available from: https://www.researchgate.net/figure/Appropriate-tunnel-catheter-position-and-anatomy_fig1_40029853 [accessed 12 Mar 2026]
Mechanism How It Works Best Removes
Diffusion Solutes move down a concentration gradient Small molecules (urea, creatinine, potassium)
Convection Solutes move with water flow (solvent drag) Middle molecules and larger solutes
Modality Mechanism
CVVH Convection
CVVHD Diffusion
CVVHDF Diffusion + Convection
Filter: HF20
Dialysis fluid: Prismasate 4K, 2.5 Ca
Replacement fluid: Prismasol 4K, 2.5 Ca
BFR: 80-100 ml/min; start with 80 ml/min and advance as tolerated
DFR: 250 ml/hr
Pre-replacement fluid rate: 200 ml/hr
Post-replacement fluid rate: 50 ml/hr
Fluid removal: Net +10 ml/hr
Dialysis replaces two major kidney functions:
Kidney's function Dialysis Equivalent
Volume regulation (i.e. urine/water) Ultrafiltration (UF) Solute clearance and balance Dialysis (diffusion and/or convection)
Ultrafiltration (UF) removes water.
Dialysis removes solutes (urea, potassium, etc.)
A typical PD exchange consists of three phases.
Phase Description
Fill: Dialysate infused into peritoneal cavity
Dwell: Diffusion and ultrafiltration occur
Drain: Used dialysate removed